


What is Gynecomastia?
Gynecomastia is also referred to informally as ‘gyno’ and ‘bitch tits’. Gynecomastia is the name for the medical disorder whereby men will experience the growth of breast tissue (hence why it is referred to as ‘bitch tits’, and that its shape and form often resembles the breast tissue of a female dog). Although on females the development of breast tissue is considered a normal occurrence as a part of the female physiology, this is not the case for males where breast tissue development and formation should not occur. The truth is that gyno can develop on a male body as a result of many different factors and causes, ranging from environmental causes to an imbalance of endogenous hormones as a result of aging. In this case, however, the Gynecomastia that is of concern is anabolic steroid induced Gynecomastia. Whatever the original cause may be, whether it is pubertal Gynecomastia, environmental Gynecomastia, or anabolic steroid related Gynecomastia, the central problem of the entire matter is the imbalance of hormones. In particular, it is the imbalance of androgens and estrogens in the body, whereby a significant increase in Estrogen is observed to be the sole cause of the issue.
In such a case, Estrogen acts as the primary culprit in the formation and the development of gyno where it will attach to the Estrogen receptors located on cells within breast tissue and signal growth. What results is then a gradual development of fatty tissue, fibrous tissue, and glandular tissue that eventually over time will formulate full Gynecomastia. Although there are various pathways of receptor up regulation and interaction with other hormones (such as Prolactin and Progesterone/Progestins), Estrogen is the central hormone and the key hormone involved in the development of Gynecomastia. It is imperative to understand that the imbalance of hormonal levels in the body that favors high levels of Estrogen is the result of aromatization, which is the conversion of aromatizable androgens (such as Testosterone or Dianabol) into Estrogen by the aromatase enzyme. However, not all anabolic steroids are capable of aromatization and many can be utilized without fear of rising Estrogen levels. It so happens, however, that the most commonly utilized and effective anabolic steroids are also aromatizable into Estrogen in at least some amount or rate. With this being said, the rate of aromatization can be different among different compounds. For example, Testosterone aromatizes at a moderate rate compared to Equipoise’s (Boldenone’s) low rate of aromatization.
With various small exceptions, it is the aromatization of various anabolic steroids that is generally exclusively the cause of high estrogen:androgen ratios in the body, which then increases the chances and likelihood of the user developing gyno. It is also very important to understand that while some individuals might never experience Gynecomastia with the use of any anabolic steroids at any dose, there are those who are extremely sensitive to Gynecomastia as the result of rising Estrogen levels. This is due to individual personal response and genetics, of which every person is different, and hence why every person will react differently to anabolic steroid or drug use of any kind.
 Signs, Symptoms, and Development Stages of Gynecomastia
Signs, Symptoms, and Development Stages of Gynecomastia
Gynecomastia of any type carries the exact same signs and symptoms of development. The signs and symptoms of Gynecomastia are very unmistakable and can be very prominent and significant. Gyno will generally progress in progressive stages, and the speed at which it will progress through these can vary due to many different factors. The intensity and severity of gyno through these stages also vary quite a bit, and there is no single general rule that can be applied to everyone concerning the development of gyno. The factors that play a role in the development of Gynecomastia that determine the speed of development and the intensity and severity of the formation of breast tissue include: the type of anabolic steroid(s) utilized, doses of anabolic steroids used, duration of use of the anabolic steroids, and perhaps the most important influential determining factor, individual personal genetics and responsiveness. The degree to which an individual responds to rising levels of Estrogen, as previously mentioned, can be very different from many others.
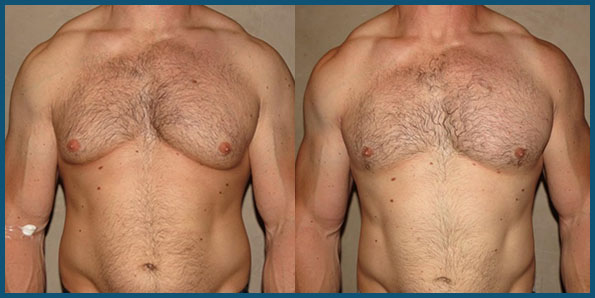
Physically, gyno can form on either side of the chest at any one time and does not have to develop equally on both sides of the chest. Many individuals will frequently experience one side of the chest ‘flare up’ with gyno while the other side exhibits no Gynecomastia development. This is quite common, and is nothing out of the ordinary for those who might be expecting Gynecomastia to formulate equally on the chest at the same time. The areola (circular region surrounding the nipple) will typically expand and look ‘puffy’, usually accompanied with a particular sensitivity (tender to the touch). Following this, some fatty tissue in and beneath the nipple might possibly be forming. The various stages of gyno development are as follows:
1. The nipple area (or slightly beneath it) is sensitive and painful to the touch.
2. Puffiness and swelling of the nipple region occurs. The development of Gynecomastia at this point is superficial with no glandular tissue development, noting that this is the reversible stage of development.
3. Complete development of gyno occurs, whereby glandular growth has become significant alongside significant fatty tissue growth. Gynecomastia at this stage is irreversible and surgery is the only viable option for removal.
Depending on the hormonal environment in the body, any aggravating factors, and other issues will determine the speed of progression through these three development stages. Some individuals might experience a rapid onset of development that completes all three stages within a matter of days, while another individual might possibly find a very slow progression over weeks, or that perhaps progression will halt at a certain stage and not move forward (perhaps in the middle of development even). Various cases of Gynecomastia can become ‘stuck’ in any of the three particular stages for months even, and if left unchecked it can sometimes regress randomly or suddenly jump in progression.
Treatment and Prevention of Gynecomastia
Both treatment as well as prevention of gyno share the same methods and techniques, with prevention expressing an additional method that simply involves the manipulation of the use of anabolic steroids during the cycle so as to avoid excessive aromatization. An ounce of prevention is indeed worth a pound of cure. The preventative measures shared with treatment measures involve the use of various anti-estrogen compounds such as SERMs (Selective Estrogen Receptor Modulators) and AIs (Aromatase Inhibitors). These must first be explained before specifically venturing into the preventative and treatment measures.
SERMs are normally the first line of defense against Gynecomastia, as these compounds will selectively block the action of Estrogen on receptors in certain tissues, namely breast tissue. The SERM, such as Nolvadex (Tamoxifen), will occupy the receptor site located within the cells of breast tissue so that Estrogen itself cannot bind to these receptors, thus blocking Estrogen’s activity. It is very important to understand very clearly, however, that SERMs such as Nolvadex do not serve to reduce total circulating Estrogen levels in the body – they simply block Estrogen’s activity in various tissues. The compounds responsible for the reduction of total Estrogen levels in the body are aromatase inhibitors (AIs) such as Arimidex (Anastrozole) and Aromasin (Exemestane). These particular compounds will compete for binding affinity to the aromatase enzyme, whereby the aromatase enzyme will bind to the AI and become rendered useless, effectively inhibiting it. As a result, the aromatase enzymes that are now inhibited cannot freely aromatize Testosterone (or any other aromatizable androgens) into Estrogen. Seeing as though this is the male human body’s method of generating Estrogen, AIs will effectively reduce total circulating levels of Estrogen so that there might be very little or no Estrogen present to cause Gynecomastia to develop.
The use of an AI at a low and/or infrequent dose throughout a cycle is a good preventative measure for the avoidance of gyno, so as to ensure that androgens used are not aromatized too significantly so as to present problems with the development of Gynecomastia. SERMs can also be used at a low dose (20mg daily of Nolvadex, for example) to chronically block the activity of Estrogen in breast tissue, but normally the former method (using an AI at a low dose during cycle) is the preferred method, as when properly employed it will maintain normal physiological levels of Estrogen. For example, a full dose of Aromasin (Exemestane) is too much and might reduce Estrogen levels too much, so therefore a dose of 12.5mg every other day is normally sufficient to keep Estrogen levels under control as opposed to totally eliminated.
For the treatment of Gynecomastia, the immediate use of a SERM (such as Nolvadex at 40mg/day) is necessary alongside the immediate full-dose use of an aromatase inhibitor (such as Aromasin at 25mg/day). The SERM should effectively be able to block the activity of Estrogen at the cellular level while the AI serves to reduce total circulating levels of Estrogen in the body. Note that this will only prevent or reduce Gynecomastia if it has not progressed beyond the second stage. If full Gynecomastia development has resulted by the time treatment has begun, then the chances become more likely that surgery is the only possible solution for removal of gyno.